


MR Shoulder
Common Histories / Key Words: Rotator Cuff Tear, Labral Tear, Shoulder Pain, Instability, Dislocation
POSITIONING: Patient supine with arm parallel to side, resting on pad (see below for ABER).
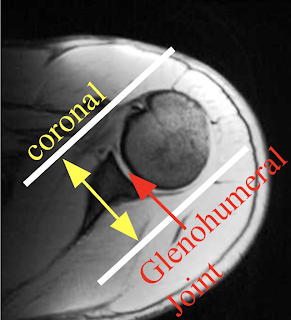
CORONAL - Set up slices perpendicular to the glenohumeral joint. Area of coverage is depicted below.
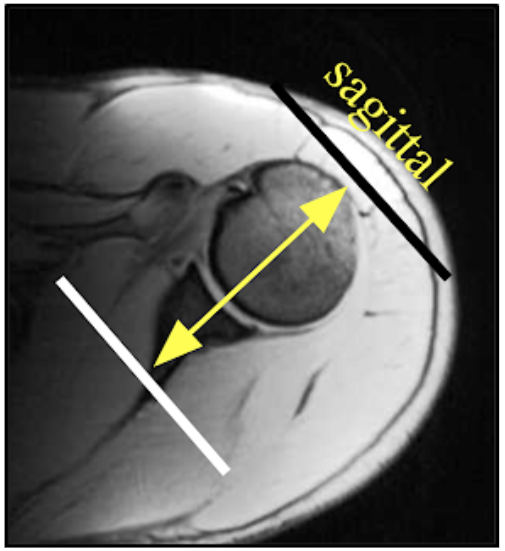
SAGITTAL - Parallel to the glenohumeral joint (perpendicular to the coronal sequence). Coverage should include from the lateral 1/3rd of the scapula through the greater tuberosity.
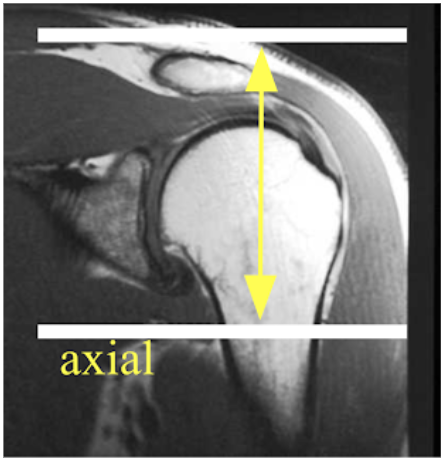
AXIAL - Coverage should include the acromioclavicular (AC) joint to below the glenohumeral joint
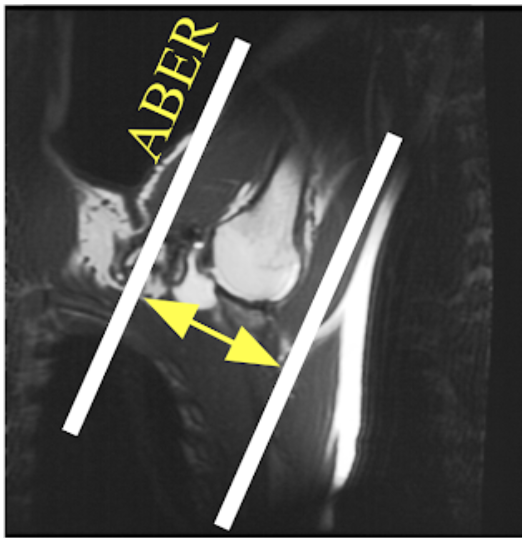
ABER (Abduction External Rotation) - Acquire coronal localizer first. Then acquire ABER T1 fat sat sequence by orienting the plane of imaging parallel to the humerus as seen below (scan medial to lateral). The ABER sequence is performed during shoulder arthrography only. This sequence is especially useful with history of dislocation and/or instability to evaluate for inferior labral tear.

ROUTINE
■ Cor T2 FS
■ Sag T1, T2 FS
■ Ax PD FS
ARTHROGRAM
■ Cor T1 FS, T2 FS
■ Sag T1 (NO FS), T2 FS
■ Ax T2 FS
■ ABER T1 FS (only with history of Dislocation, Instability, Bankart, Labral Tear)
Please see
MR MASS - INFECTION - ALL JOINT/EXTREMITIES
link for post IV contrast protocol
METAL ARTIFACT - STIR sequences may be substituted in place of T2 FS when metal artifact is present in attempt to improve signal and image quality. Please see link below for additional suggestions.
■ MR METAL ARTIFACT